
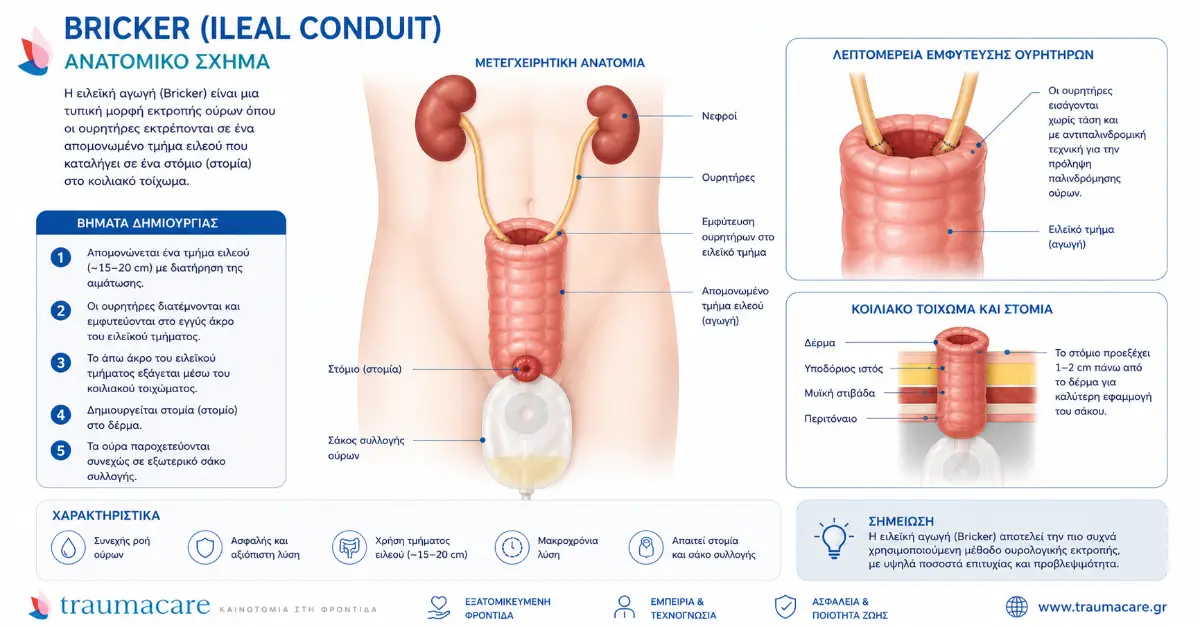
What is the Bricker technique
The Bricker ureteroenterodermostomy (known internationally as ileal conduit ) is the most common method of urinary diversion after radical cystectomy — accounting for over 60% of urinary diversion procedures worldwide [1] . The technique was first described in 1950 by Eugene Bricker in Surgical Clinics of North America [2] and remains the gold standard 75 years later — because it is technically simple, safe, and suitable for a wide range of patients.
In this article we explain the entire process: from preoperative preparation to discharge and return to daily life.
Stage 1: Preoperative preparation (2-4 weeks before)
According to the EAU Guidelines 2024 for muscle-invasive bladder cancer [1] , proper preparation includes:
- Oncological staging: CT/MRI of the upper abdomen and pelvis, bone scan, lymph node evaluation.
- Renal function: eGFR, creatinine, electrolytes — eGFR > 45 mL/min for safe ileal conduit.
- Cardiological and anesthesiological assessment: ECG, echo, respiratory function.
- Stoma siting: By a qualified stoma nurse — critical step. Correct positioning affects the adherence of the pouch for the patient’s entire life.
- Bowel prep: Bowel cleansing with osmotic medication 1 day before, according to the ERAS protocol.
- Nutrition and hygiene: Protein supplementation 7-14 days before, smoking cessation (ideally 4 weeks) [3] .
- Selection of stoma materials: Discussion with supplier — here we recommend B Braun Flexima Uro Silk for flat stomas, Active O' convex for retracted/flush.
Stage 2: Surgery (4-7 hours)
Radical cystectomy with ileal conduit creation is performed under general anesthesia and lasts 4-7 hours depending on the technique (open, laparoscopic, or robotic). In modern high-volume clinics, the robotic approach (RARC — robot-assisted radical cystectomy) is increasingly used, although ileal conduit construction is often performed extracorporeally [3] .
The 6 basic steps of the procedure
| Step | What is done | Duration |
|---|---|---|
| 1 | Access and exploration: mid-lower abdominal incision or robotic trocar. Liver inspection, lymph nodes, assessment of local tumor extent. | ~30 minutes |
| 2 | Pelvic lymphadenectomy: removal of pelvic lymph nodes (obturator, internal iliac, external iliac) for staging. | 60-90 minutes |
| 3 | Radical cystectomy: removal of the bladder (in men together with the prostate and seminal vesicles, in women with the uterus and anterior vaginal wall in some cases). | 90-120 minutes |
| 4 | Intestinal loop isolation: selection of a 15-20 cm segment of the terminal ileum, ~15 cm from the ileocolic valve. Preservation of vascularity (mesenteric pedicle). | 30 minutes |
| 5 | Ureteroileal anastomosis (Bricker or Wallace): union of the two ureters at the posterior end of the ileal loop. Either separately (Bricker), or united in a plate (Wallace). | 45-60 minutes |
| 6 | Stoma: the anterior end of the loop is brought out through the abdominal wall at a preoperatively marked position, forming an evertable nipple stoma 1-2 cm high. | 30 minutes |
Ureteral stents are placed into the anastomoses and removed through the stoma — they are left in place for 10–14 days to allow the suture to heal without pressure.
Stage 3: Hospitalization (5-10 days)
According to current ERAS protocols and large cohort data, the average length of hospital stay is 7-9 days — but depends on the patient's course [3] .
- Days 1-2: ICU or post-anesthesia care unit — mobilization, breathing exercises, IV fluids, analgesia.
- Days 3-5: Gradual resumption of feeding (clear fluids → full). Stoma nurse begins bag change training.
- Days 6-9: Full mobilization, independent bag change, discharge.
- Days 10-14: Ureteral stents removed in the office.
The Memorial Sloan Kettering study of 1,142 patients [4] showed that approximately 64% of patients experience some postoperative complication in the first 90 days—although serious complications (Clavien Grade III+) are relatively rare (~13%). Modern ERAS techniques further reduce the rates.
Stage 4: Home Recovery (Weeks 2-12)
Full recovery takes 3 months . In the first 6 weeks:
- The stoma changes shape — it starts out swollen and gradually shrinks. Different sizes of flanges will be needed.
- No heavy lifting (over 5 kg) for 6 weeks — risk of parastomal hernia.
- No swimming or hot baths for 4 weeks (although showers are allowed after the 1st week).
- Bag change: every 3-5 days with Flexima — see detailed article on urostomy bag change .
The systematic review by Cookingham et al. (2022) in World Journal of Urology [5] shows that quality of life (HRQoL) in patients with ileal conduit is comparable to that of patients with neocystic kidney after the first 6-12 months of adaptation. Many patients return to work and activities.
Selection of materials after surgery
In the first 4-6 weeks, the right choice of bag makes the difference for:
- Protection of peristomal skin (the skin is sensitive in the first weeks)
- Prevention of urinary tract infections (anti-reflux valve)
- Psychological adaptation (discreet appearance under clothes)
At Traumacare, as exclusive representatives of B Braun Avitum in Greece , we recommend:
| Stage | Flexima Recommendation |
|---|---|
| Weeks 1-4 (bulging stoma) | Flexima Uro Silk Flat larger size, with midi beige cover |
| Weeks 4-12 (reducing stoma) | Re-sizing — possible change to Convex if retraction is present |
| After 3rd month (stable stoma) | Permanent system: Flexima Uro Silk (flat) or Active O' convex accordingly |
Full EOPYY coverage: According to the Government Gazette B' 5395/09-10-2025 [6] , EOPYY covers 270€/month urostomy materials with 0% patient participation. Traumacare handles the entire process (e-EOPYY, pickup, next-day delivery).
Complications to be aware of
According to BAUS (British Association of Urological Surgeons) data [7] :
- Early (first 30 days): ileus 10-15%, surgical wound infection ~10%, renal dysfunction ~5%, deep vein thrombosis 2-3%.
- Late (after 3 months): parastomal hernia 15-30% (increasing with age), stoma stenosis 5-10%, kidney stones 5-10%, hydronephrosis 5%.
- Rare: incidental calcification, metabolic acidosis from intestinal absorption.
Regular follow-up with a urologist every 3-6 months for the first two years, and annually thereafter, is critical for early detection of complications [1] .
Book a pre-operative consultation
| ✉️ Contact form | 💬 Viber channel Traumacare ✓ |
Related articles
- What is ureterostomy — cutaneous vs ileal conduit
- When is a ureterostomy done — indications
- Comparison: Nephrostomy vs Ureterostomy vs Neocyst
- How do I change a urostomy bag — steps
Author: Vangelis Micharikopoulos, Traumacare — exclusive representatives of B Braun Avitum Greece
Scientific documentation: EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer (2024), AUA/ASCO/SUO Guideline on MIBC (2017, amended 2024), Bricker EM Surg Clin North Am 1950, Stein JP J Clin Oncol 2001, Shabsigh A Eur Urol 2009, BAUS Patient Information
Last updated: May 2026
Note: The content is for informational purposes only and is not a substitute for medical advice. Always consult your healthcare professional for individual decisions.
📚 Bibliography / Scientific sources
- EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer . European Association of Urology, 2024. uroweb.org/guidelines
- Bricker EM. Bladder substitution after pelvic evisceration . Surgical Clinics of North America , 1950;30(5):1511-1521. PMID: 14782163. pubmed.ncbi.nlm.nih.gov
- AUA/ASCO/SUO Guideline on Muscle-Invasive Bladder Cancer . American Urological Association, 2017 (amended 2024). auanet.org
- Shabsigh A et al. Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology . European Urology , 2009;55(1):164-176. pubmed.ncbi.nlm.nih.gov
- Cookingham LM et al. Health-related quality of life in patients with ileal conduit urinary diversion: a systematic review . World Journal of Urology , 2022. pubmed.ncbi.nlm.nih.gov
- ΦΕΚ Β' 5395/09-10-2025 — Definition of stoma materials with EOPYY coverage . National Printing House. eopyy.gov.gr
- BAUS — Information about Urinary Diversion (Ileal Conduit) . British Association of Urological Surgeons. baus.org.uk
- UOAA — United Ostomy Associations of America: Urostomy Guide . ostomy.org/urostomy
- Stein JP et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients . Journal of Clinical Oncology , 2001;19(3):666-675. pubmed.ncbi.nlm.nih.gov