
Ureterostomy (or urinary diversion ) is not a “forced solution” — it is a life-saving treatment option when the bladder needs to be removed or bypassed. In this article, we explain in which medical conditions it is recommended, which patients are suitable candidates, and what you should know before making the surgical decision.
The main indication: Bladder cancer
In the vast majority of cases (approximately 75-80%), ureterostomy is performed after radical cystectomy for muscle-invasive bladder cancer (MIBC).
Radical cystectomy is standard-of-care when:
- The tumor has invaded the muscularis mucosae of the bladder ( stage T2 or higher )
- There are recurrent high-risk non-invasive tumors (CIS, T1 high-grade) that are not responsive to BCG
- The tumor is multifocal or to the point where partial cystectomy is not feasible
According to the current guidelines of the European Urological Association ( EAU 2024 ), after cystectomy the patient has three basic options for urinary diversion:
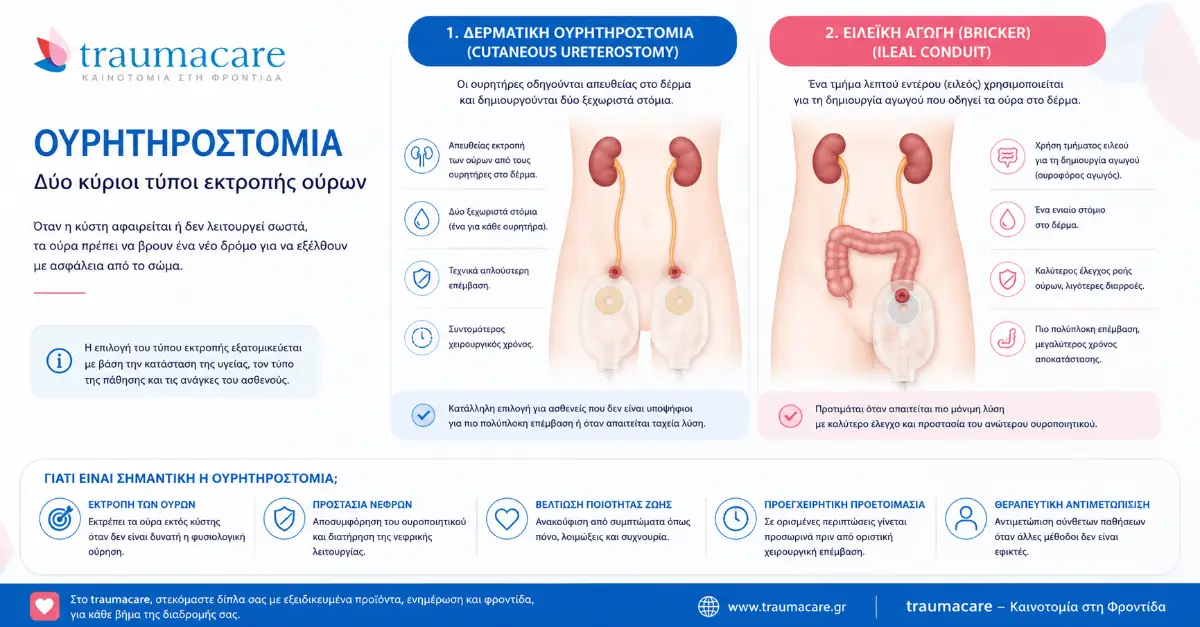
- Ileal Conduit (Bricker): the most common and technically simple option — this article is about
- Orthotopic neocyst: new bladder from the intestine, with preservation of normal urination through the urethra
- Continuous cutaneous diversion (e.g. Indiana pouch): reservoir without continuous outflow, with self-catheterization every 4-6 hours
The ileal conduit (Bricker) ureterostomy remains the most common option worldwide (above 60% of cystectomies), because it is technically simpler, has a lower postoperative risk, and is suitable for a wider range of patients—even the elderly or those with comorbidities.
Other (non-cancerous) indications
In 20–25% of cases, ureterostomy is performed for non-oncological reasons . The most important indications are:
| Condition | Why ureterostomy is required |
|---|---|
| Neurogenic bladder (spinal cord injury, multiple sclerosis) | When self-catheterization or medications fail and there is imminent renal damage from high bladder pressures. |
| Severe radiation cystitis | After pelvic radiotherapy with chronic bleeding and pain that are not controlled conservatively. |
| Complex urogenital fistulas (vesicovaginal, vesicorectal) | When fistula repair has repeatedly failed or there is extensive tissue damage. |
| Chronic incontinence refractory to all treatments | Very rare indication — only when it severely impairs quality of life and all other interventions have been exhausted. |
| Congenital anomalies (pediatric, e.g., bladder exstrophy, spastic neurogenic) | When the anatomy or function of the bladder does not allow normal urination and there is a risk to the kidneys. |
| Invasive gynecological tumor | In advanced cervical or ovarian cancer with bladder invasion, as part of pelvic exenteration. |
When is ureterostomy preferred over neocystectomy?
Many patients ask: “ Why did my doctor recommend an ileal conduit and not a neocystectomy? Isn't the neocyst better so I can urinate normally? »
The truth is that the neocyst is not "better" — it is different . It has strict eligibility criteria and its selection depends on:
- Age and general condition: Patients over 75 or with significant comorbidities are less likely to tolerate the major neocyst surgery.
- Renal function: for neocyst an eGFR > 45 mL/min is required — otherwise metabolic disturbances become uncontrolled.
- Urethral and sphincter function: If the sphincter is damaged or there is tumor infiltration of the urethra, neobladder is not feasible.
- Ability to self-catheterize: 25–30% of patients with neobladder require intermittent self-catheterization for complete voiding. Not all patients are willing or able to do this.
- Psychological adjustment: Neobladder requires 6–12 months of voiding training—with possible nocturnal incontinence and the need for scheduled voiding.
In contrast, Bricker-type ureterostomy is suitable for almost all patients who require cystectomy — and offers safety, low postoperative risk, and predictable care.
Pediatric indications
In children, ureterostomy (usually cutaneous ureterostomy , without an intestinal loop) is used:
- In spastic neurogenic bladder from spina bifida (myelomeningocele), as a temporary solution until the child can be a candidate for augmentation.
- In incidental dilatation of the renal pelvis with hydronephrosis that threatens renal function.
- In congenital anatomical anomalies (PUV — posterior urethral valves with severe renal damage).
In pediatric cases, ureterostomy is often temporary — it can be reversed when the child grows older and the condition improves.
What happens before the surgery
When you make the decision for a ureterostomy, preparation begins at least 2-4 weeks before. The main steps:
- Urological and oncological staging (scintigraphy, CT, MRI as appropriate).
- Stoma marking by a specialized stoma nurse — the ideal position of the stoma on the abdomen is selected before surgery (away from bony prominences, folds, belt, navel).
- Psychological preparation — discussion with a specialist or other patients who have gone through the same procedure.
- Selection of materials — and here comes the most important part for your daily life afterwards.
Selection of a ureterostomy bag: why it matters now
In the first 4-6 weeks after surgery, the stoma changes shape — it starts out swollen and gradually gets smaller. This means that you will need different bags at different stages. Choosing the right materials from day one makes all the difference.
At Traumacare, as exclusive representatives of B Braun Avitum in Greece , we recommend the Flexima series — because:
- ✅ Anti-reflux valve — prevents urine from refluxing into the stoma (crucial for avoiding urinary tract infections)
- ✅ Hydrocolloid skin protector — does not irritate the skin even in the first sensitive weeks
- ✅ Soft convexity options — for stomas that have entered the skin (retracted) or are flat (flush)
- ✅ Midi beige discreet cover — not visible under clothes
- ✅ German manufacturing — reliability, quality materials, stable adhesion for 3-5 days
- ✅ 100% EOPYY coverage (270€/month, 0% participation) — with the new Official Gazette B' 5395/09-10-2025
Book a pre-operative information appointment
| ✉️ Contact form | 💬 Viber channel Traumacare ✓ |
In the consultation we will discuss:
- The type of surgery you will have (cutaneous vs ileal conduit)
- How the pouch will change in the first 6 weeks
- Which Flexima is right for you (flat, convex, midi cover)
- How the EOPYY procedure is done (medical opinion, e-EOPYY)
- What supplies to have ready at home after discharge
Related articles
- What is ureterostomy — cutaneous vs ileal conduit
- Bricker / Ileal Conduit: the surgical procedure step by step
- Comparison: Nephrostomy vs Ureterostomy vs Neocyst
- Pillar: Complete guide to ureterostomy