
“I have a lump around my stoma — what is it?”
Parastomal hernia is the most common late complication of colostomy. According to current data [1] :
- 15-30% of patients in the first 2 years
- ~38% at 5 years
- >50% in patients living with a colostomy for more than 10 years
It is almost inevitable statistically — but proper prevention and early recognition can dramatically reduce symptoms and avoid surgical reoperation.
What is a Parastomal Hernia
When a colostomy is created, the surgeon makes an opening in the abdominal muscles to bring the intestine out to the skin. This opening is a weak point. Over time, intestinal tissue or fatty tissue can protrude through this gap, creating a visible bulge around the stoma [2] .
How to Recognize
Main Symptoms [3] :
- Bulging around the stoma, especially when standing or squeezing the abdomen
- The bulge decreases when lying on your back
- Difficulty attaching pouch — leaks around the stoma
- Feeling of heaviness or discomfort in the area
- Mild pain especially after heavy lifting or physical exertion
- In advanced stages: visible swelling under clothing
Test you can do at home: Stand in front of a mirror and tighten your stomach (as if you were coughing). If you see a bulge around the stoma that is clearly protruding, you may have a parastomal hernia. Confirmation is made by a surgeon with a clinical examination and possibly an abdominal CT scan [4] .
⚠️ When to Seek Immediate Medical Care
Risk Factors
According to the study by Donahue et al. (2014) [5] and the EHS Guidelines:
| Factor | Role |
|---|---|
| Obesity (BMI >30) | Major factor — doubles the risk |
| Age >65 years | Reduced tissue elasticity |
| Chronic cough / COPD | Persistent intra-abdominal pressure |
| Constipation | Abdominal tightness, chronic pressure |
| Smoking | Affects collagen synthesis |
| Corticosteroids / immunosuppression | Delayed healing |
| Surgical wound infection | Poor muscle healing wall |
| Early heavy exercise | Lifting more than 5 kg before complete healing |
🛡️ Prevention: The 6 Basic Measures
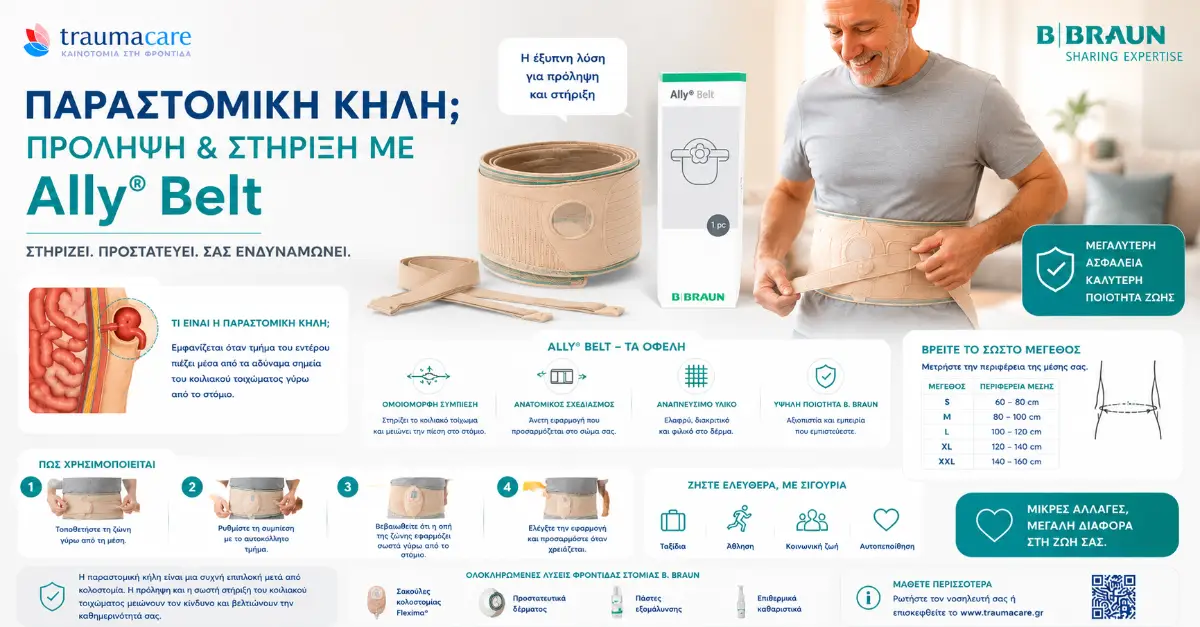
1. ⭐ Ally Belt Support Belt (Strategy No.1)
The Ally Belt by B Braun is the most proven effective conservative means for:
- ✅ Prevention (in high-risk patients: obese, elderly, COPD)
- ✅ Management of small parastomal hernias (retains hernia without surgery)
- ✅ Exercise & heavy work — protects the abdominal wall
- ✅ After hernia repair — protects the surgical repair
Ally Belt Features:
- Comfortable, breathable, adjustable
- Special hole for the stoma so you can wear a Flexima bag underneath
- Hypoallergenic fabric — does not irritate the skin
- 100% covered by EOPYY (1 pc/6 months, 290€/month in total for all colostomy materials) [6]
2. Mesh Prophylaxis during Surgery (Primary Prevention)
According to the Donahue et al. study and recent RCTs [5] , prophylactic mesh placement during radical colostomy reduces the incidence of parastomal hernia by >50% at 5 years. It is recommended by the EHS Guidelines for high-risk patients.
If you are preoperative, discuss with your surgeon whether you are at high risk (BMI >30, age, COPD) so that he or she can consider the option.
3. Stable Weight/Weight Loss
Maintaining a normal BMI (<25) is the most modifiable risk factor. In obese patients, a loss of >10% of body weight can reduce risk by >30%.
4. Proper Core Strengthening Exercises
According to the guidelines of UOAA [7] :
- ❌ AVOID: sit-ups, planks, lifting weights >5 kg, crunches
- ✅ ALLOWED (always with Ally Belt): light walking, breathing exercises, gentle pelvic exercise, swimming
5. Cough and Constipation Management
- Quitting smoking — reduces cough and improves collagen healing
- COPD medications — controls cough
- High-fiber diet — prevents constipation
- Mild laxatives if needed
6. Proper Lifting Technique
- Bend the knees, not the waist
- Keep the object close to the body
- Exhale on lifting — do not hold your breath (Valsalva maneuver increases intra-abdominal pressure)
- Wear Ally Belt before any physical exertion
Diagnosis: How It Is Made
According to ESCP Guidelines [8] :
- Clinical examination — standing, lying, with Valsalva (abdominal tightening). Often sufficient for diagnosis.
- Contrast-enhanced abdominal CT scan — gold standard, reveals size, content, and potential complications. Recommended when surgical planning is needed.
- Abdominal ultrasound — alternative, less accurate but radiation-free.
🛡️ Conservative Management (>70% of cases)
Most parastomal hernias do not require surgery. Conservative approach includes:
| Solution | How it helps |
|---|---|
| ⭐ B Braun Ally Belt | Daily use during physical activity — holds hernia |
| Flexima Active O' Convex | Convex base that adapts to uneven hernia surface |
| B Braun Ally Paste | Filling of skin defects for sealing |
| Change of technique | Application in supine position (where hernia is reduced), not standing |
| Regular follow-up | Visit every 6 months to a surgeon for progress assessment |
Surgical Treatment (When Necessary)
Surgical repair of a parastomal hernia is indicated when [9] :
- There are persistent leaks that are not corrected by bag changes
- Severe pain or discomfort that affects quality of life
- Episodes of incarceration (hernia that does not return)
- Emergency: hernia strangulation
- Aesthetic reasons (large visible swelling that affects psychologically)
Types of Surgery Repair
| Technique | Features |
|---|---|
| Primary suture repair | Simple suture — high recurrence rate (50-70%). Used only in urgent cases. |
| Sublay mesh repair | Mesh under the abdominal muscles. Recurrence 15-25%. |
| Keyhole / Sugarbaker laparoscopic | Laparoscopic mesh approach. Current option — recurrence 10-20%. |
| Stoma relocation | Stoma relocation to a new location. Option for refractory cases — but new hiatus may present with new hernia. |
The Cochrane Review confirms that mesh repair is superior to simple suturing in reducing recurrence [1] .
Living with a Parastomal Hernia
Many patients live with a small or moderate parastomal hernia for years without the need for surgery. With proper Ally Belt, proper Flexima Convex pouch, and regular follow-up, quality of life is maintained.
What else can you do:
- ✅ Office work, driving, traveling
- ✅ Light to moderate cardio (walking, cycling, swimming)
- ✅ Sex life
- ⚠️ With caution: gym exercise (always with Ally Belt)
- ❌ Avoid: lifting weights >10 kg, sit-ups, contact sports
Try Ally Belt + Flexima Convex for free
| ✉️ Request a free sample | 💬 Viber Traumacare ✓ |
Related articles
- Pillar C: Complete guide to colostomy
- Bag Leakage — 7 Causes & Solutions
- Colostomy Bag: Which One Should I Choose?
- Exercising & Traveling with a Colostomy
Author: Traumacare Medical Group — exclusive representatives of B Braun Avitum in Greece
Scientific documentation: Antoniou SA et al. EHS Guidelines on parastomal hernias 2018, Donahue TF et al. J Urology 2014 (Risk factors), ESCP Guidelines, ASCRS Clinical Practice Guidelines, Cochrane Review on parastomal hernia repair, ΦΕΚ Β' 5395/09-10-2025
Last updated: May 2026
Note: In case of sudden severe pain, swelling that does not return, nausea/vomiting, or cessation of bowel movements, go to the emergency room IMMEDIATELY. Possible hernia strangulation requires urgent surgical treatment.
📚 Βιβλιογραφία / Επιστημονικές πηγές
- Antoniou SA et al. European Hernia Society guidelines on prevention and treatment of parastomal hernias . Hernia , 2018. pubmed.ncbi.nlm.nih.gov
- BAUS — Information about Parastomal Hernia . British Association of Urological Surgeons. baus.org.uk
- Liu NW et al. Risk factors for parastomal hernia following radical cystectomy with ileal conduit . Urologic Oncology . pubmed.ncbi.nlm.nih.gov
- ASCRS Clinical Practice Guidelines for the Surgical Care of Patients with Colostomy . American Society of Colon and Rectal Surgeons. fascrs.org
- Donahue TF et al. Risk factors for the development of parastomal hernia after radical cystectomy . Journal of Urology , 2014;191(6):1708-1713. pubmed.ncbi.nlm.nih.gov
- ΦΕΚ Β' 5395/09-10-2025 — Πίνακας 11, Α/Α 2 (Υλικά Κολοστομίας — περιλαμβάνει Ζώνη Στομίας 1 τμχ/6 μήνες) . Εθνικό Τυπογραφείο. eopyy.gov.gr
- UOAA — United Ostomy Associations of America: Hernia Prevention & Management . ostomy.org
- ESCP Guidelines on Parastomal Hernias . European Society of Coloproctology. escp.eu.com
- Cochrane Review: Surgical mesh for parastomal hernia repair . Cochrane Database of Systematic Reviews. cochranelibrary.com